SARS-CoV-2 Antigen Rapid Test Cassette

Short Description:
The SARS-CoV-2 Antigen Rapid Test Cassette is a rapid chromatographic immunoassay for the qualitative detection of SARS-CoV-2 antigen in human Oropharyngeal swabs.The identification is based on the monoclonal antibodies specific for the Nucleocapsid (N) Protein of SARS-CoV-2.It is intended to aid in the rapid differential diagnosis of COVID-19 infection.
INTENDED USE
The SARS-CoV-2 Antigen Rapid Test Cassette is a rapid chromatographic immunoassay for the qualitative detection of SARS-CoV-2 antigen in human Oropharyngeal swabs.The identification is based on the monoclonal antibodies specific for the Nucleocapsid (N) Protein of SARS-CoV-2.It is intended to aid in the rapid differential diagnosis of COVID-19 infection.
Package Specifications
25 tests/pack, 50 tests/pack, 100 tests/pack
INTRODUCTION
The novel coronaviruses belong to β genus.COVID-19 is an acute respiratory infectious disease.People are generally susceptible.Currently, the patients infected by the novel coronavirus are the main source of infection;asymptomatic infected people can also be an infectious source.Based on the current epidemiological investigation,the incubation period is 1 to 14 days, mostly 3 to 7 days. The main manifestations include fever, fatigue and dry cough. Nasal congestion,runny nose,sore throat, myalgia and diarrhea are found in a few cases.
REAGENTS
The test cassette contains anti-SARS-CoV-2 Nucleocapsid protein particles and anti-SARS-CoV-2 Nucleocapsid protein coated on the membrane.
PRECAUTIONS
Please read all the information in this package insert before performing the test.
1.For professional in vitro diagnostic use only. Do not use after the expiration date.
2.The test should remain in the sealed pouch until ready to use .
3.All specimens should be considered potentially hazardous and handled in the same manner as an infection agent.
4.The used test should be discarded according to local regulations.
5.Avoid using bloody samples.
6.Wear gloves wen handing the samples,avoid touching the reagent membrane and sample well.
STORAGE AND STABILITY
The validity period is 18 months if this product is stored in an environment of
2-30℃.The test is stable through the expiration date printed on the sealed pouch.The test must remain in the sealed pouch until use.DO NOT FREEZE.Do not use beyond the expiration date.
SPECIMEN COLLECTION AND PREPARTION
1.Throat secretion collection: Insert a sterile swab into the throat completely from the mouth, centering on the throat wall and the reddened area of the palate tonsils, wipe the bilateral pharyngeal tonsils and posterior pharyngeal wall with moderate
force, avoid touching the tongue and take out the swab.
2.Process the sample immediately with sample extraction solution provided in the kit after the sample is collected. If it cannot be processed immediately, the sample should be stored in a dry, sterilized and strictly sealed plastic tube. It can be stored at 2-8℃ for 8 hours , and can be stored for a long time at -70℃.
3. Samples that are heavily contaminated by oral food residues cannot be used for testing of this product. Samples collected from swabs that are too viscous or agglomerated are not recommended for testing of this product. If the swabs are contaminated with a large amount of blood, they are not recommended for testing. It is not recommended to use the samples that are processed with sample extraction solution not provided in this kit for testing of this product.
KIT COMPONENTS
Materials provide
Materials required but not provide
Specifications25
tests/pack50
tests/pack100
tests/packSample Extraction Reagent25 tests/pack50 tests/pack100 tests/packSample extraction
tube≥25 tests/pack≥50 tests/pack≥100 tests/packInstructionRefer to the
packageRefer to the
packageRefer to the
package
DIRECTIONS FOR USE
Allow the test, specimen, extraction buffer to equilibrate to room temperature(15-30℃) prior to testing .
1.Remove the test cassette from the sealed foil pouch and use it within 15 minutes. Best results will be obtained if the assay is performed immediately after opening the foil pouch.
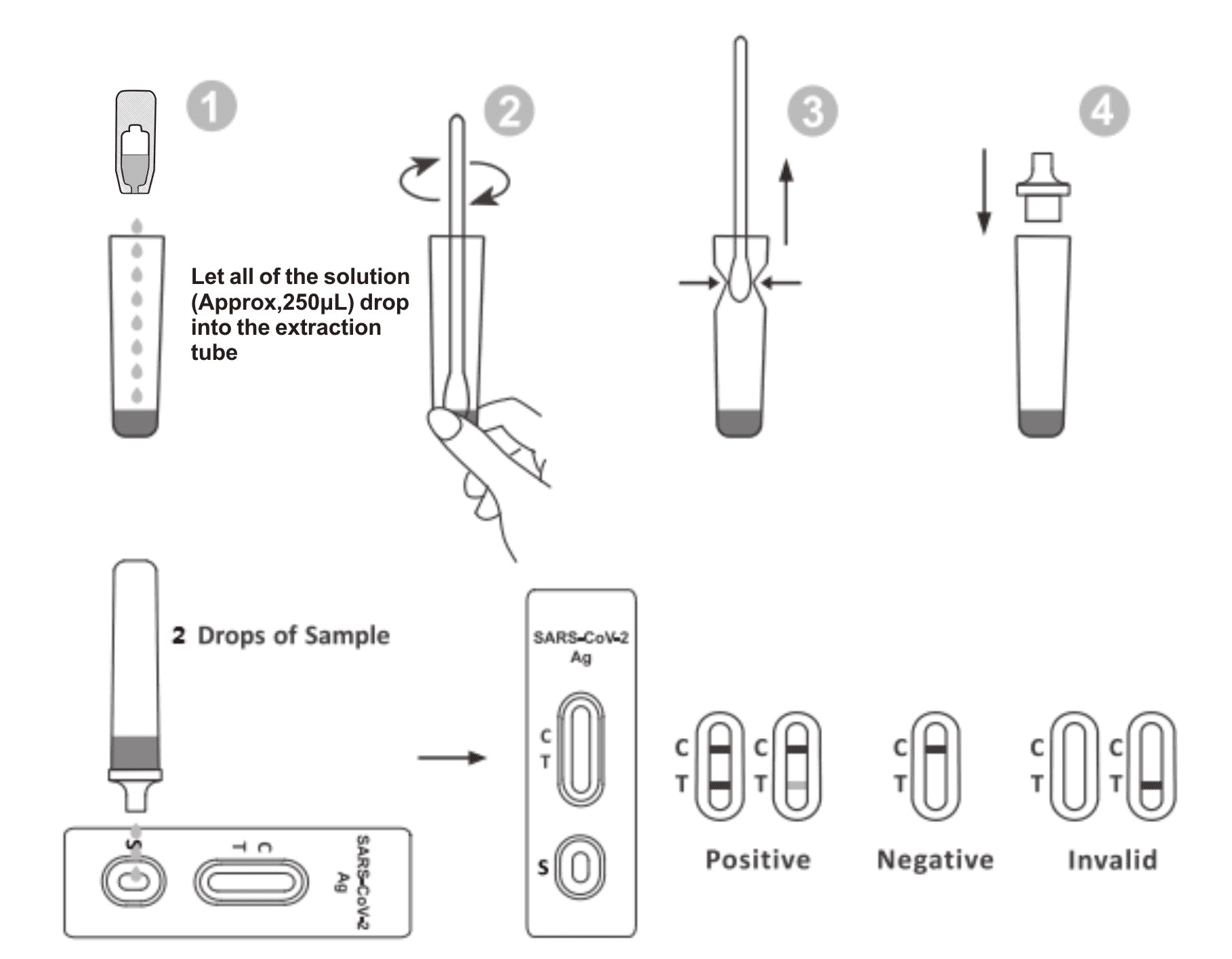
2.Place the Extraction Tube in the work station.Hold the extraction reagent bottle upside down vertically.Squeeze the bottle and let all of the solution (Approx,250μL) drop into the extraction tube freely without touching the edge of the tube to the Extraction Tube.
3.Place the swab specimen in the Extraction Tube.Rotate the swab for approximately 10 seconds while pressing the head against the inside of the tube to release the antigen in the swab.
4.Remove the swab while squeezing the swab head against the inside of the Extraction Tube as you remove it to expel as much liquid as possible form the swab.Discard the swab in accordance with your biohazard waste disposal protocol.
5.Fit the dropper tip on top of the extraction tube.Place the test cassette on a clean and level surface.
6.Add 2 drops of the solution(approx,65μL) to the sample well and then start the timer.Read the displayed result within 20-30 minutes, and the results read after 30 minutes is invalid.
INTERPRETATION OF RESULTS
One colored line appears in the control line region (C). No line appears in the test region (T).A negative result indicates that SARS-CoV-2 antigen is not present in the specimen,or is present below the detectable level of the test.
POSITIVE RESULT:
Two lines appear.one colored line should be in the control region (C) and another apparent colored line should be in the test region (T).A positive result indicates that SARS-CoV-2 was detected in the specimen.
INVALID RESULT:
Control line fails to appear.Insufficient specimen volume or incorrect procedural techniques are most likely reasons for control line failure. Review the procedure and repeat the test with a new test. If the problem persists, discontinue using the test kit immediately and contact your local distributor.
NOTE:
The intensity of the color in test line region (T) will vary depending on the concentration of SARS-CoV-2 Antigen present in the specimen. Therefore, any shade of color in the test line region(T) should be considered positive.
QUALITY CONTROL
- A procedural control is included in the test. A colored line appearing in the control region(C) is considered an internal procedural control.It confirms adequate membrane wicking.
- Control standards are not supplied with this kit; however, it is recommended that positive and negative controls be tested as a good laboratory practice to confirm the test procedure and to verify proper test performance.
LIMITATIONS OF THE TEST
- The SARS-CoV-2 Antigen Rapid Test Cassette is for professional in vitro diagnostic use only.The test should be used for the detection of SARS-CoV-2 Antigen in Oropharyngeal Swab.Neither the quantitative value nor the rate of increase in SARS-CoV-2 concentration can be determined by this qualitative test.
- The accuracy of the test depends on the quality of the swab sample.False negatives may result form improper sample collestion storage.
- The SARS-CoV-2 Antigen Rapid Test Cassette will only indicate the presence of SARS-CoV-2 in the specimen from both viable and non-viable SARS-CoV-2 coronavirus strains.
- As with all diagnostic tests,all results must be interpreted together with other clinical information available to the physician.
- A negative result obtained from this kit should be confirmed by PCR.A negative result may be obtained if the concentration of the SARS-CoV-2 present in the swab is not adequate or is below the detectable level of the test.
- Excess blood or mucus on the swab specimen may interfere with performance and may yield a false positive result.
- A positive result for SARS-CoV-2 does not preclude an underlying co-infection with anther pathogen. Therefore the possibillity of an unerlying bacterial infection should be considered.
- Negative results do not rule out SARS-CoV-2 infection,particularly in those who have been in contact with the virus. Follow-up testing with a molecular diagnostic should be considered to rule out infection in these individuals.
- Positive results may be due to present infection with non-SARS-CoV-2 coronavirus strains,such as coronavirus HKU1,NL63,OC43,or 229E.
- Results from antigen testing should not be used as the sole basis to diagnose or exclude SARS-CoV-2 infection or to inform infection status.
- Extraction reagent has the ability to kill the virus , but it cannot inactivate 100% of the virus.The method of inactivating the virus can be referred to: what method is recommended by WHO/CDC,or it can be handled according to local regulations.
PERFORMANCE CHARACTERISTICS
Sensitivity and Specificity
The SARS-CoV-2 Antigen Rapid Test Cassette has been evaluated with specimens obtained from the patients.PCR is used as the reference method for the SARS-CoV-2 Antigen Rapid Test Cassette.Specimens were considered positive if PCR indicated a positive result.
Relative Sensitivity :95.0%(95%CI*:83.1%-99.4%)
Relative Specificity:99.2%(95%CI*:97.6%-99.8%)
*Confidence Intervals
Detection Limit
When the virus content is greater than 400TCID 50 /ml, the positive detection rate is greater than 95%. When the virus content is less than 200TCID 50 /ml, the positive detection rate is less than 95%, so the minimum detection limit of this product is 400TCID 50 /ml.
Precision
Three consecutive batches of reagents were tested for precision. Different batches of reagents were used to test the same negative sample 10 times in succession, and the results were all negative. Different batches of reagents were used to test the same positive sample 10 times in succession, and the results were all positive.
HOOK effect
When the virus content in the sample to be tested reaches 4.0*105TCID50/ml, the test result still does not show the HOOK effect.
Cross-Reactivity
Cross-reactivity of the Kit was evaluated. The results showed no cross reactivity with the following specimen.
Interfering Substances
The test results do not be interfered with the substance at the following concentration:
IBIBLIOGRAPHY
1.Weiss SR,Leibowitz JZ.Coronavirus pathogenesis. Adv Virus Res 2011;81:85-164
2.Cui J,Li F,Shi ZL.Origin and evolution of pathogenic coronaviruses.Nat Rev Microbiol 2019;17:181-192.
3.Su S,Wong G,Shi W,et al.Epidemiology,genetic recombination,and pathogenesis of coronaviruses. TrendsMicrobiol 2016;24:490-502.

